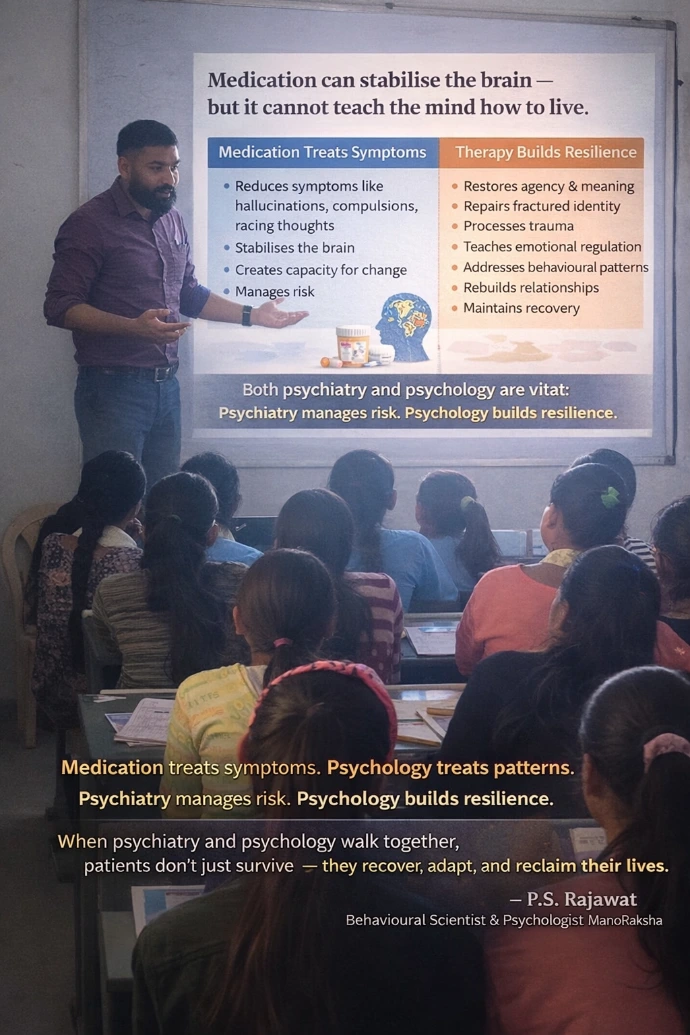
Medication can stabilise the brain, but it cannot teach the mind how to live...!!
There are phases of illness where medication is essential, even life-saving.
Psychosis, severe mania, acute suicidality ... these are not moments for insight-oriented work.
The brain must be stabilised first. No disagreement there.
But here is what is often left unsaid 👇
🔶 Stabilisation is not recovery.
Medication can reduce hallucinations, slow racing thoughts, lift mood, or quiet compulsions.
What it cannot do is:
- repair fractured identity
- process trauma
- rebuild meaning
- relearn relationships
- restore agency
- teach emotional regulation
- address behavioural patterns that maintain relapse
Once the brain is calm enough to engage, psychological work becomes indispensable.
Consider this:
👉 Two people on identical medication, with identical diagnoses — only one receives structured psychological intervention.
Over time, outcomes diverge. Relapse rates diverge. Functioning diverges. Quality of life diverges.
Why?
Because mental illness is not just brain chemistry gone wrong.
It is also:
- lived experience
- learning history
- attachment wounds
- cognitive schemas
- environmental stressors
- social conditioning
🔶 Medication treats symptoms. Psychology treats patterns.
🔶 Psychiatry manages risk. Psychology builds resilience.
🔶 Medication creates capacity. Therapy teaches utilisation.
Without psychological intervention:
- patients remain dependent on dosage changes
- insight remains shallow
- compliance becomes fragile
- recovery remains incomplete
This is complementarity.
The most ethical, evidence-based mental health care recognises:
🧠 Neurobiology sets the stage
🧩 Psychology writes the script
When psychiatry and psychology walk together, patients don’t just survive —
they recover, adapt, and reclaim their lives.
Dr. P. S. Rajawat
Behavioural Scientist & Psychologist
ManoRaksha
.
Start writing here...